Case Presentation:
A 52-year-old male with metastatic cancer undergoing chemotherapy presented to the Emergency Department with:
● Acute chest pain
● Shortness of breath
Vital signs:
● Respiratory Rate: 26
● O₂ Saturation: 94% (on room air)
● Blood Pressure: 100/65 mmHg
● Heart Rate: 111 bpm
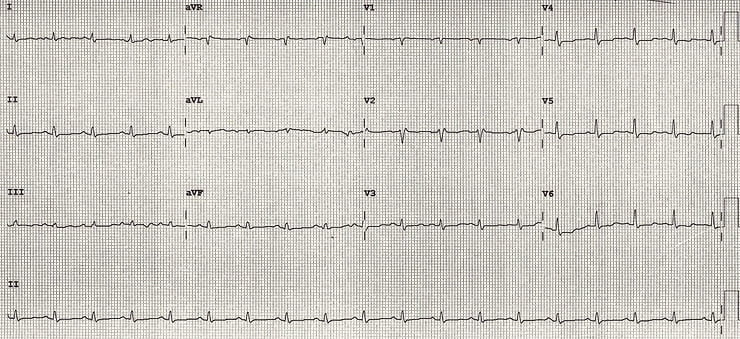
This was the ECG of the patient,
What is your diagnosis?
What is your diagnosis?
Let’s walk through the case as it unfolded in real time.
First Impression: Suspected Pulmonary Embolism
The initial clinical picture strongly suggested PE:
● Active cancer
● Ongoing chemotherapy
● Sudden chest pain + SOB
● Tachypnea and tachycardia
He fit every box for anticoagulation and admission with planned CT Pulmonary Angiogram (CTPA)
But one key detail almost derailed everything…

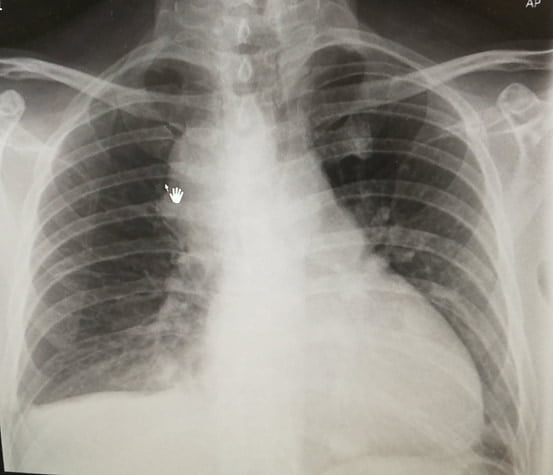
Chest X-Ray Clue
Although the CXR was AP view, cardiomegaly was evident.
This raised concern — and led to a closer look at the ECG.
- ECG Findings
- ECG Findings
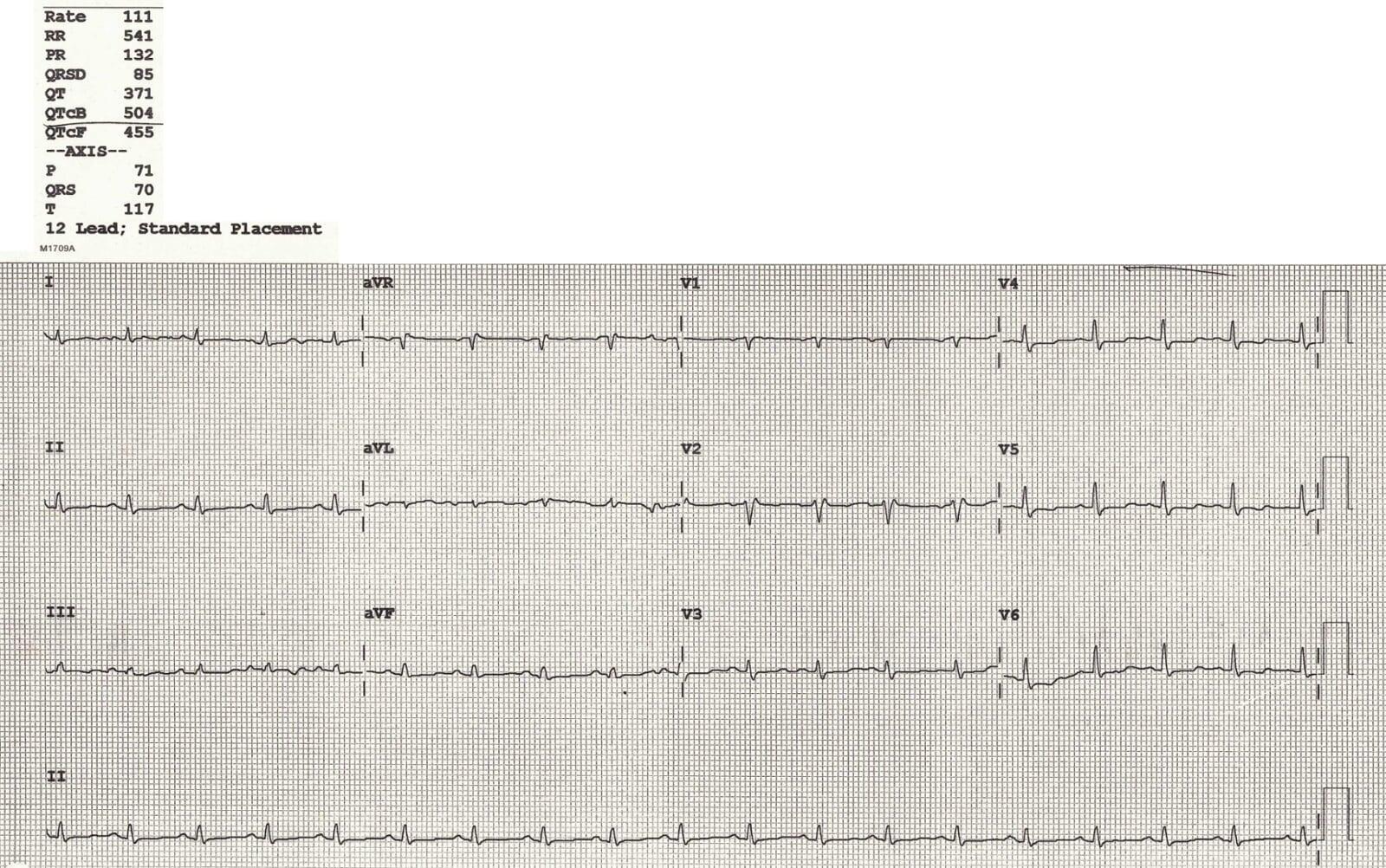
The ECG showed two critical abnormalities:
- About the Long QT
- Focus: Low Voltage ECG
1. Prolonged QTc
2. Low voltage ECG
● Likely related to chemotherapy
● Electrolytes were not severely abnormal
● Will be covered in detail in another blog
Definition:
● Limb leads (I + II + III) total height < 15 small squares, and/or
● Precordial leads (V1–V3) total height < 30 small squares
Causes fall into two categories:
1) Poor signal generation by the heart:
● Cardiomyopathy
● Hypothyroidism
● Myocardial infiltration (e.g. sarcoidosis)
2) Barriers between the heart and leads:
● Fat (obesity)
● Air (COPD)
● Fluid (pericardial/pleural effusion)
- Pattern Recognition: Tachycardia + Low Voltage
- Pattern Recognition: Tachycardia + Low Voltage
💡 This combination strongly suggests:
Pericardial Effusion
Classic ECG Triad of Massive Pericardial Effusion:
● Low Voltage ECG
● Tachycardia
● Electrical Alternans(not seen in this case)
- Why This Matters?
- Why This Matters?
If this patient had been anticoagulated for presumed PE, he may have deteriorated due to hemorrhagic tamponade from undiagnosed pericardial effusion.
- What Was Done?
- What Was Done?
● Immediate bedside echo was performed → Confirmed pericardial effusion
● CTPA was expedited (to rule out PE before anticoagulating)
● CTPA showed no pulmonary embolism
🟢 Patient was safely admitted to CCU and did well.
- Key Learning Points:
- Key Learning Points:
● Low-voltage ECG is a powerful early clue
● Tachycardia + Low Voltage = Think pericardial effusion
● Don’t treat presumed PE blindly — stop and confirm
● CTPA + Echo combo is crucial when the diagnosis is unclear
Below are the Echo findings of this patient
- 🔗 Further Learning
- 🔗 Further Learning
✅ FAQ – Small, Yet Dangerous
Q1: What are the ECG criteria for diagnosing low voltage?
A1: Limb leads I + II + III < 15 mm combined, or V1–V3 < 30 mm combined.
Q2: What should you consider when dealing with low voltage ECG with tachycardia?
A2: Pericardial effusion is the most serious cause, especially in cancer patients or those with inflammatory conditions.
Q3: Why is anticoagulating blindly in suspected PE dangerous?
A3: In cases like pericardial effusion, anticoagulation may lead to hemorrhagic tamponade and death.
Want to take your ECG reasoning even further?
If this case grabbed your attention, the Emergency Physician’s ECG Course (EPEC) builds on exactly this type of real clinical problem solving, with live teaching, interpretation frameworks, and patterns you’ll use day in, day out in the ED.
Learn how to consistently read tough ECGs with confidence, not guesswork.