
Case Presentation
A 46-year-old male patient with a high BMI and a history of paraplegia secondary to an old spinal cord injury was discovered on the floor by his carer in the early morning. It’s unclear how long he remained there, but it was likely overnight.Upon assessment, the patient appeared confused, though hemodynamically stable. Blood work revealed Acute Kidney Injury (AKI), likely due to rhabdomyolysis from prolonged immobility.
Can you guess what the reason was for the abnormalities in this ECG?
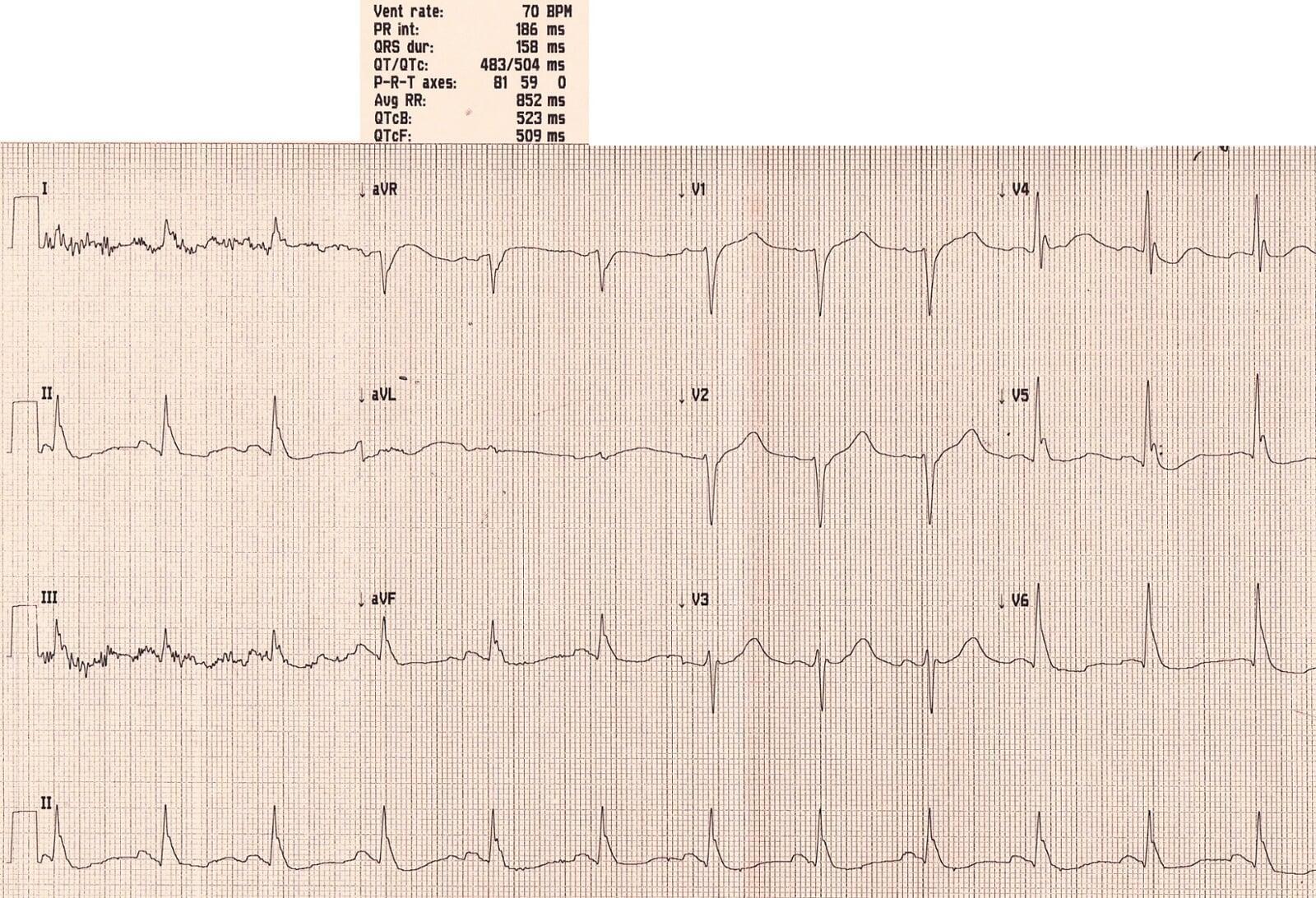
Initial ECG Findings
“Can you guess what caused the ECG abnormalities?”
1. Prolonged QTc (QTc = 523 ms)
This is a critical red flag. A prolonged QTc can have several causes:
Causes of QTc Prolongation
- Congenital
Romano-Ward syndrome
- Metabolic (All the Hypo’s):
Hypokalemia (K)Hypocalcemia (Ca)Hypomagnesemia (Mg)HypothermiaHypothyroidism
- Medications:
Tricyclic antidepressants (TCA), AmiodaroneAntipsychotics, AntidepressantsAntihistamines, OndansetronMacrolides (e.g., Clarithromycin)Methadone
- Other:
Increased Intracranial Pressure (ICP)
Acute Coronary Syndrome (ACS)
A Common ED Trap
Imagine a young patient with mental health conditions presenting to the ED with a chest infection and nausea.
They receive Amoxicillin + Clarithromycin and Ondansetron—a recipe for disaster if they’re already on antidepressants or antipsychotics.
Without an ECG, a dangerously prolonged QTc could go unnoticed, putting the patient at serious risk for ventricular tachycardia (VT).
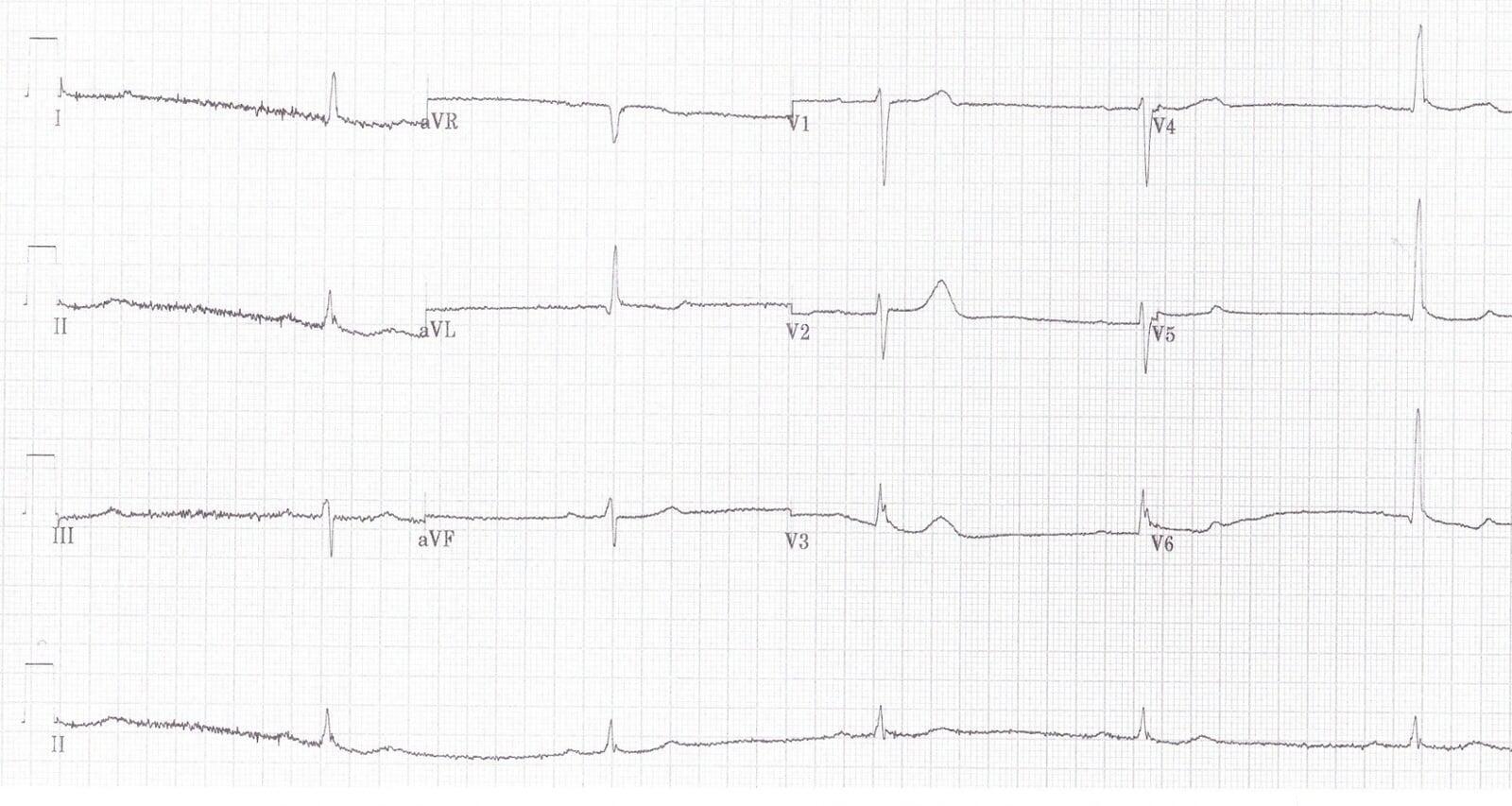
Osborn Waves (J-Waves)
A distinctive wave at the end of the ECG complex stood out:
- Positive in positive complexes
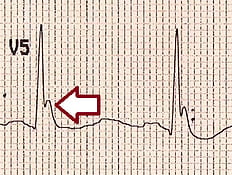
- Negative in negative complexes
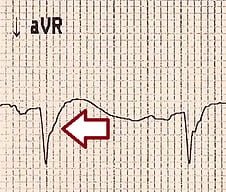
Known as Osborn Waves, these occur as deflections at the J-point, most visible in leads V2–V6, and are classically linked to:
Hypothermia
Hypercalcemia
Raised ICP
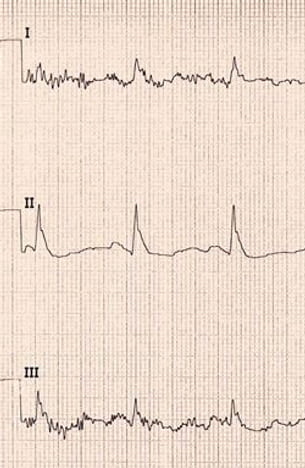
Shivering Artifacts
Movement artifacts were noted in leads I and III, consistent with shivering.
Diagnosis: Hypothermia
Combining:
QTc prolongation
Osborn waves
Shivering artifacts
ECG should not replace core temperature measurement, but can provide valuable diagnostic clues in emergency settings.
ECG Changes in Hypothermia
1. Prolonged PR, QRS & QT intervals
2. Bradyarrhythmias (e.g., sinus bradycardia, slow AF)
3. Osborn (J) waves — may mimic STEMI
4. Shivering artifacts
5. Ventricular ectopics
Additional ECG Examples
A hypothermic patient mimicking STEMI (Case courtesy: Tom Cromwell, UK)
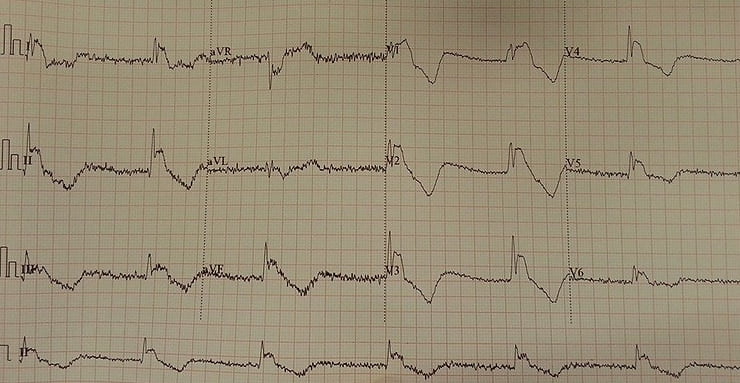
Temperature at 28°C with all hallmark findings
Key Takeaways
Always consider hypothermia in confused patients with prolonged QTc and Osborn waves.
Be vigilant about QTc-prolonging drug combinations in emergency care.
ECG remains a critical, rapid, and informative tool for diagnosing underlying systemic conditions.
Always consider hypothermia in confused patients with prolonged QTc and Osborn waves.
Be vigilant about QTc-prolonging drug combinations in emergency care.
ECG remains a critical, rapid, and informative tool for diagnosing underlying systemic conditions.
✅ FAQ Section for This Article
Q1: What are the ECG signs of hypothermia?
A1: ECG signs of hypothermia include prolonged PR, QRS, and QT intervals, Osborn waves (J-waves), shivering artifacts, bradyarrhythmias, and ventricular ectopics.
Q2: What are Osborn waves, and when do they appear?
A2: Osborn waves are positive deflections at the J-point, often seen in hypothermia, hypercalcemia, or increased intracranial pressure (ICP).
Q3: what can cause the QT interval to be prolonged" or something similar?
A3: A prolonged QTc can result from metabolic imbalances, medications, congenital syndromes, or conditions like hypothermia and should be carefully correlated with clinical context.
Q1: What are the ECG signs of hypothermia?
A1: ECG signs of hypothermia include prolonged PR, QRS, and QT intervals, Osborn waves (J-waves), shivering artifacts, bradyarrhythmias, and ventricular ectopics.
Q2: What are Osborn waves, and when do they appear?
A2: Osborn waves are positive deflections at the J-point, often seen in hypothermia, hypercalcemia, or increased intracranial pressure (ICP).
Q3: what can cause the QT interval to be prolonged" or something similar?
A3: A prolonged QTc can result from metabolic imbalances, medications, congenital syndromes, or conditions like hypothermia and should be carefully correlated with clinical context.
🔗 Further Reading
- Pericardial Effusion ECG Case: Low Voltage Misdiagnosed as Pulmonary Embolism “Small, Yet Dangerous"
See you in the next case — check out Ventricular Tachycardia vs Movement Artifacts: ECG Clues You Shouldn’t Miss to sharpen your ECG interpretation skills.
- Pericardial Effusion ECG Case: Low Voltage Misdiagnosed as Pulmonary Embolism “Small, Yet Dangerous"
See you in the next case — check out Ventricular Tachycardia vs Movement Artifacts: ECG Clues You Shouldn’t Miss to sharpen your ECG interpretation skills.
Want to take your ECG reasoning even further?
If this case grabbed your attention, the Emergency Physician’s ECG Course (EPEC) builds on exactly this type of real clinical problem solving, with live teaching, interpretation frameworks, and patterns you’ll use day in, day out in the ED.
Learn how to consistently read tough ECGs with confidence, not guesswork.